Mass struggle at the university hospital in Rome: experience of an autonomous collective
You can read a short summary about the struggles that are described in the book here and watch a documentary here. Translating this inspiring book seems worthwhile for two reasons. Firstly, at least in the English-speaking world there is little historical material about autonomous communist working class organisation in Italy in the 1960s and 1970s that does not focus on either factories or the question of reproduction. Secondly, despite the fact that the times and conditions have changed, we can still learn a lot from these experiences. The book inspires us as we plan to organise a revolutionary hospital workers’ newspaper and collective in 2024. Watch this space!
Nicoletta Stame (1940) collaborated in ‘Classe e Stato’, ‘Quaderni Piacentini’, ‘Vento dell’Est’. Francesco Pisarri (1946) is a medical doctor and has worked at the university hospital. They both participated in the ‘Centro stampa comunista di Roma’.
Introduction
1. This book documents an inquiry into a recent struggle that expressed some of the most significant ideas that our movement has developed: it is about a struggle against class medicine and for the proletarian management of a hospital in which the workers on the Policlinico Umberto I in Rome have been involved in since 1971.
Even though there has been a lot written about this dispute in the local media, there are only a few comrades who know what actually happened at the Policlinico. This struggle has bothered plenty of people: the authorities of the government, of the regional administration, of the university and hospital hierarchy, the barons of the university and the clinic bosses, the directors of the pharmaceutical industry, as well as the communist party PCI and the trade unions; everyone of them, each according to the role they play, haven’t missed any opportunity to accuse the workers (branded as ‘extremists’, ‘provocateurs’, ‘slackers’ – depending on the case) and to confuse the public opinion about the real significance of the struggle. Even many comrades were influenced by this big deployment of bourgeois propaganda. This is why we feel the need to understand what has moved the workers to become active and to analyse their actions.
As soon as we approached the comrades who led the struggle, the main principles of their initiative became apparent: we were facing one of those rare cases in which the proletarians themselves lead a struggle for health without delegating this neither to the official organisations of the left nor to the progressive bourgeois technicians. By basing itself on those who expressed the most ‘radical’ needs (“To be radical is to grasp things by the root. But for man the root is man himself.”) [1] and by relating the particularity of the ‘medical oppression’ constantly to the general proletarian condition in our society, they managed to develop a mass line which became the stronghold of workers and patients united against the barons of medicine [2], their common enemy, and to snatch from the latter – apart from important victories – also the mask of power.
Another significant reason for the achieved successes of their initiative, together with various subjective and objective factors that we try to explain in this book, was the capacity that the workers who were organised in the Workers’ Collective of the Policlinico developed to engage in continued inquiries into their own situation, into the relations of production to which they are subjected to and into the mass needs. They made use of these inquiries to verify their political line and as a stimulus for the conscious participation of the masses in transformative action. Rejecting revisionist politics that tries to make workers believe that the ideas of the bourgeoisie are their own ideas, the workers made an effort to clarify which are their own ideas, their own needs, their own reasons in order to make them the basis of their own politics.
2. It seems that in order to study these experiences we need to develop instruments of political inquiry to be able to grasp the anti-capitalist and anti-revisionist significance that the masses have given their struggle.
We know how difficult it is for workers in a, what is usually defined as, ‘mass society’ to develop their own ideas, to break through the smoke screen that is created by all those who speak of ‘the masses’, who engage in research ‘into the masses’ or act ‘in the name of the masses’. We also know that amongst comrades of intellectual or petit-bourgeois background, who constitute a fair share of our organised movement and who don’t have a deeper knowledge about the way of life and thought of the popular masses, the revisionist ideas which seem to stem from inside the masses themselves (whereas actually they are formulated within the official ‘workers’ organisations), and therefore seem to be the most progressive, are also the ones that spread most easily. It is therefore a pressing task to clarify also for ourselves which are these revisionist ideas that we intended to contest with our inquiry.
A first idea relates to the property relations within the health service, which is divided into a public and a private sector. The revisionists maintain that the struggle against the medical barons, who are representative of a clientelist, mafia-like and parasitic power, can only try to subordinate the private sector to public management with the desire to reform the latter; as a result we would have an ‘efficient’, ‘rational’ and ‘modern’ system that would solve all our problems. In this way you don’t question the class contradictions that emerge from within the labour process [processo produttivo] and the class interest of the workers is confused with ‘public management’ of the institutions; and most importantly, you don’t manage to clearly recognise the new public ‘regime’ of property as the enemy of the masses.
A second revisionist idea, which is related to the first, states that within the health service you cannot struggle without harming the patients, unlike in the manufacturing sectors of goods, where the struggle harms the bosses. This argument is based on a willful mystification: the workers who are excluded from exercising any power when it comes to the management of the public institutions (because they would not have the ‘expertise’ or ‘capacity’) are at the same time considered to be the only ones that are responsible when it comes to the functionality of the service. If you don’t understand that the struggle for health has to attack the class relations that develop within the labour process of the health sector, you will inevitably end up pandering to the interests of those who actually dominate these relations entirely (who certainly are not the sick ‘users’).
A third revisionist idea claims that if the general interest is to obtain reforms that put the health service under public management then the sole task of the workers becomes to strengthen the trade union that fights for this policy. In this way, “anyone who is against the trade union is either a fascist or an infiltrator”, or at least a “corporatist”. This is the idea that has perhaps the strongest influence amongst many comrades, who might agree with the arguments of the previous two assumptions, but who think that the trade union is the “historical organisation of the working class” and that if you don’t want to detach yourself from the masses it is necessary to avoid detaching yourself from the union. In this way, many of these comrades who have approached the struggle ended up with the following judgement: “the workers fought a just fight as long as they were combatting the bosses, but once they became sectarian towards the trade union, they could only end up remaining isolated”.
In a preliminary way these are the interpretations of the situation that we are opposing. [3] Even if we often repeat that the masses are the real heroes, that without the masses we are nothing, very little is actually done to put the masses – the scientific analysis of their ideas, of their capacity to comprehend the reality that surrounds them – at the centre of the elaboration of a political line. This means that little is done to confront the class contradictions and the division of manual and intellectual labour on which the capitalist society thrives. Consequently there is a persistent tendency within the political line of our movement to have an open flank for revisionism.
To become aware of the necessity to combat this tendency meant realising that also in our case it is not enough to simply preach that “who doesn’t engage in inquiry has no right to speak” in order to obtain a correct style of working [4], but that it becomes a moment in the struggle between opposed political lines. [5]
We therefore propose to follow the workers in their process of forming a consciousness of the various aspects of hospital reality (from the first struggles in small groups to the big mass struggles and beyond) in order to understand how class relations develop in concrete terms within the hospital and in which conditions it is possible to enforce a proletarian class position in the struggle for health.
3. But things don’t become any easier once we have decided to put the masses at the centre of our inquiry. It is necessary to grasp the complexity of their situation from at least two points of view. Firstly, the popular masses cannot be understood outside of the contradictory relations that they have with the social classes that dominate them. Secondly, within the popular masses there exist diverse opinions, advanced and backward elements, revolutionary layers and attachments to the old society, and it is not possible to focus on only one of these aspects. If we are not aware of these problems it is easy to fall into the trap of unilateral analysis.
A prime error of this type is, for example, to only see the revolutionary moment of the masses, the most developed point of their consciousness, and thereby to forget that the conditions of exploitation and oppression in which the masses exist undergo a process of ‘conditioning’ of the proletariat to the rules of this system. This ‘conditioning’ is part of the ‘conditions’ which the proletariat has to take into account in order to develop its own struggle. [6] Therefore, it is necessary to understand that victories over the enemy can only be obtained through heavy battles also within our own camp, and that in the situation that follows, a new (instable) equilibrium of oppression/subordination is created which requires to prepare ourselves for fighting again and on a different plane. [7]
At this point it is also possible to commit the opposite error, which is to focus only on the contribution that all parties who are involved in the health system (both oppressed and oppressors) make for its ‘functioning’ in relation to a goal that is imposed by those in power (a goal that could be the strengthening of the power of the medical barons, the increase of the profits of the multinationals, the expansion of the public sector or even solely the creation of a sphere of consensus with the rules of the system) and the workers (as the ‘instruments’ that keep the system running). If it is true that the barons and the upper hierarchy of the hospital have managed to install a system of domination that reproduces itself on the various levels of hierarchy and that shapes the entire institution within which it exercises its power, then it is also necessary to remember that the equilibrium on which the system seems to rest is only a surface appearance, the straight-jacket of the relation of production, which the struggle of the oppressed aim to break. [8]
This conception of the social relations in the hospital, which considers the tendency towards equilibrium as primary and the struggle as secondary, can end up subsuming the mass movement to a bourgeois direction and leadership. This is, in fact, the ideological expression of a very active social strata, of democratic medical professionals. They actually are in a leading position within the struggle against the medical barons, but don’t recognise that pushing towards a proletarian leadership of the struggle for health is the coherent consequence of the negation of one’s own role as a medical professional. [9]
If the democratic medical professionals affirm that “medicine is a form of power” and that in the field of health, capital develops its political-scientific apparatus in opposition to the masses, then they cannot fight this power without without putting themselves at the service of the movement of those who have suffered this oppression up to now. If the latter don’t become active subjects in the overthrow of the baron’s medical system by using all means at their disposal (which includes the necessary alliance with the ‘specialist’ comrades), the demystification from above would end up privileging the intellectual elements of the struggle – meaning, the small and middle-bourgeoisie – and being reduced to a simple change of leadership over the ‘inert’ masses of manual workers.
On the other hand the proletariat – in order to be not only the engine, but also the leading element of the struggle – needs to know the relations of power in a concrete sense and the various points of disequilibrium that can tip the current balance of power.
With the political inquiry moving towards deeper levels, the overt stability of the system, once seen from its fundament, turns out to be a rather precarious equilibrium: what seems on the surface level as the power of the barons reveals itself to have plenty of cracks, because the weakness and impotence of the masses, and their underlying radical needs, can transform themselves into critical capacity, in a movement to “overturn the current state of things”.
It is by grasping this complex set of conditions that the proletariat can develop the strength of their autonomy and the initiative of their struggle.
Adorno, one of the sharpest critic of the ‘totalitarianism of the system’, scolds the Marxists of today for never asking the question: “how subjects who have been conditioned in such a way (the proletarians in a situation of social impotence and alienation imposed by monopolistic capital) could be capable of an action (the revolution) that does not only require intelligence, a common vision and presence of spirit, but also an capacity of extreme abnegation”. [10] The question contains a challenge and is infused with scepticism. We think that the best answer that one can give to this question is the following: situations exist in which the proletariat has proven to possess such qualities, and we have studied one of such situations. Now we have to understand its basis, its ways, its effects and prospects. This is what we propose with this book.
4. It seems that the questions that are at the centre of the struggle for autonomy led by the workers of the university clinic can be summarised in this way.
a) Workers are the material basis of everything that happens inside the hospital: they perform the heavy and dangerous tasks that the doctors don’t want to do (tasks that capital considers as ‘less important’ in relation to those which require a high degree of ‘specialisation’), and also tasks of great responsibility, such as the continuous care for patients, which requires a presence of spirit in the moment of need, capacity of initiative etc.. Furthermore, in contrast to the doctors who are never present, the workers’ presence is the only social relation – apart from the solidarity or envy that other patients express – that is offered to the patient and that keeps them in communication with the outside world and with their own class reality. These social relations are not less important for the recovery of the patients than the medical treatment that they receive.
It goes without saying that without the ‘precious collaboration’ of the workers, no specialist scientific activity could ever take place. Despite this, their activity is defined as auxiliary and the focus of attention lies on intellectual and specialised labour. From this results that they don’t hold any power; the ample space that is granted for union representation does not respond to a recognition of the role of labour, but to the need of capital to control it and to keep the masses of workers at a ‘corporative’ level. On this level one is only concerned with problems regarding the sale of ‘labour power’, rather than demanding to be valued as an essential social component for the production of a health service.
From this emerges the tendency amongst those workers who rebel against this existing state of things to try and reconstruct how the hospital functions, in order to understand to which extent and how society depends on their labour. Many of their work colleagues respond to this with a mixture of incredulity and mistrust, given the fact that they are used to not demanding anything, as they are not valued themselves. The vanguard of the workers, in contrast, look around and ask themselves who benefits from the work that is performed in a hospital – and who performs that work. They discover that even amongst them there are people who perform tasks to cure the sick and others whose work only serves the medical barons; that there are useful activities and departments that should be expanded and others that are useless and are only there to make ‘the university’ look good; that also amongst those workers who are not manual workers not everyone is a parasite or there to control other workers (it is clear that a health service is not only produced by manual workers). As these experiences and valuations unify and confront each other, workers manage to grasp the laws of movement of the entire baronal system and to evaluate the weight of their own contribution in concrete terms and without mystifications (the understanding that they perform essential labour without which the barons would be nothing provides workers with a consciousness regarding their own power, whereas realising that one’s own work just helps to control people or to serve the barons can give an important insight into the conditioning that we are subjected to by the system).
b) Even if workers are the basis of production, they don’t enjoy its fruits – and they only receive the ‘necessary wage’ from the resources that the state spends on the health sector, while others share the rest amongst them. These others – the hospital directos, the directors of administrations, the university barons and super-bureaucrats of any type – are the only public actors who appear and they appear by sharing the bulk of resources and by arguing about the criteria that this process of sharing out should take, with their own controversies, with their litigations and bickering. Only these actors are taken into account in journalistic inquiries or television programs when it comes to elaborations of improbable reform projects. Hence the interest of the workers to measure the distance between themselves and the others, which also entails to investigate these conflicts in order to understand the entire pyramide of power, which is made up by solid alliances at the top (the financial and familial connections between the medical barons, the intertwined partaking in the profits of the private clinics, mutual support between private and public entities) the attempts of corruption and cooptation of the intermediate layers (for who they concede the crumbs of the banquet) and the plundering of the lowest layer.
c) The workers are those who are closest to the proletarian patients. Like them they find themselves at the lowest level of the hospital hierarchy, they come from the same social environment, they know – also through their own experience – that a fair share of the problems of the sick have social causes, and they are the only ones who have an interest in making these social factors become more visible (in contrast to the doctors who neglect the incidents of social factors in illness, in order to have free reign to exercise their ability as specialists).
Hence the tendency amongst the workers to encourage the patients to speak, to let them participate in their assemblies, to investigate together the reasons for illness and to put the patients in a position to fight with greater strength against the oppressive experiences of the hospital.
5. The knowledge that has been gained by the workers in the course of this process has been further deepened with the struggle for the ‘proletarian management of the hospital’ and during the development of this struggle new problems have emerged and are emerging that they have to reflect upon.
At this point the reader might object and we want to respond to this possible objection immediately. One could concede that “the workers’ struggle has been interesting, but for heaven’s sake, you cannot base a whole theory on it”. Or perhaps one could think that “certain things” only happen at the Policlinico in Rome, and that this situation is unique and not comparable with other hospitals.
We think that there are real aspects within the arguments that are made in favour of the ‘uniqueness’ of the situation at the Policlinico, but if anything these aspects make the situation at the Policlinico more ‘typical’ for the current health system in our country. There is, for example, the argument that because we deal with a ‘university clinic’ it doesn’t make sense to denounce the level of care that you are given there (this is an argumentation that implicitly admits that you have to pay a price for the sake of development, without saying explicitly who is supposed to pay it).
On the contrary, we maintain that the Policlinico being a university clinic allows us to observe the ‘driving’ tendencies within modern medicine there, whose knowledge is increasingly appropriated by monopolistic capital which, in that way, positions itself against manual labour and the ‘ignorance’ of the masses. There we can observe, better than anywhere else, that the function of ‘research’ is reserved for specialists.
Others, in turn, proclaim that the success of the workers’ struggle at the Policlinico depended on the particular nature of those in power there (who are easily identifiable as enemies of the masses) and on the little space that this form of power leaves for reformist politics: the merit of the workers is thereby reduced to having benefited from this favourable situation.
It is true that the power of the medical barons is very consistent and concentrated. In Rome, the relations between economic, political and academic power – which are close everywhere – are directly linked to the decisions of the national government and therefore involve much more complex interests than in any other regional or provincial hospital. But even if this is true and if it makes the maneuvers of those in power more visible and easier to attack than in other places, it only means that here we can see ‘amplified’ what also happens elsewhere: even if there is less power to share in other places, the nature of those in power will neither be different, nor will their willingness to share power with others be greater. It is true that this intertwinement of power of the medical barons is highlighted in the health system in Rome, where a large layer of private hospitals coexists with the public health sector (with the barons as hinges at the top). But this condition exists in all regions of the country, even if not to the same proportions. [11]
As we can see, all these are not particular characteristics which would impede to confront them with the situation in other hospitals or which would invalidate the significance of the workers’ struggle at the Policlinico, but rather they are concrete aspects of the development of the mode of production of health services in post-war Italy. [12]
In our opinion the argumentation has to be put on its feet. One cannot understand this struggle if one doesn’t refer to the current general political situation in this country. The struggle at the Policlinico is integral part of the movement that developed in Italy in 1968: the students against the academic powers, the workers against various aspects of the capitalist mode of production, the popular masses against the mafia-clientelist regime of the christ-democrat government and against US imperialism. All these aspects are also verifiable within the struggle against the barons of the university, who centralise all these forms of power that are being criticized by the mass movement. It is not by chance that hospitals are one of the strongholds of the regime that has prospered with the Christ-Democrat government; due to the increased need for health care of the population, hospitals have grown excessively and have contributed to the social politics of the monopoly bourgeoisie: they have become centres for the formation of a clientele for high-ranking Christ-Democrats, they have played a role in controlling the labour market through recruitment policies, they have contributed to the formation of an intermediate social layer that is entrusted with a role of social stabilisation.
These are elements that the new ‘democratic leadership’ of the region and the hospitals inherits and that it uses to affirm its new power. And although we are not able to tell why movements of this type didn’t also develop in other situations, or rather, why they only start to develop now, (we would need concrete and detailed analysis for that), it is clear that the only particular factor in this struggle was the capacity of those comrades who have led the struggle to use the contradictions of the situation as a lever (contradictions that we also see in other hospitals), with the aim to impact on those subjective elements that could emerge in this phase: the decline of the power of the barons, the real strength of the masses once they manage to overcome the divisions and fear. We can say that, despite many difficulties, in this case the proletarian leadership never failed. In the first place, workers were always clear about the fact that by attacking the parasitism of the barons you don’t remove cancer from an otherwise ‘healthy’ ‘public’ health system, but you rather attack a crucial aspect of the entire system in order to fight it better in future. In the second place, by withdrawing power from the barons workers were in a position to impede that their own problems were solved in a corporative fashion, that the divisions between patients and workers deepened, that the general interest in health provisions were sacrificed for particular interests (such as, for example, for efficiency, which is so dear to certain careerist doctors).
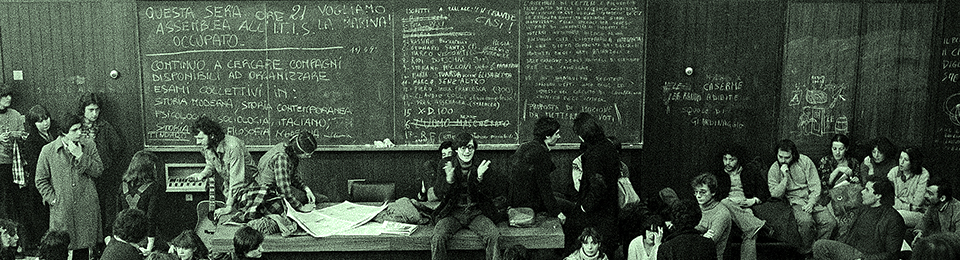
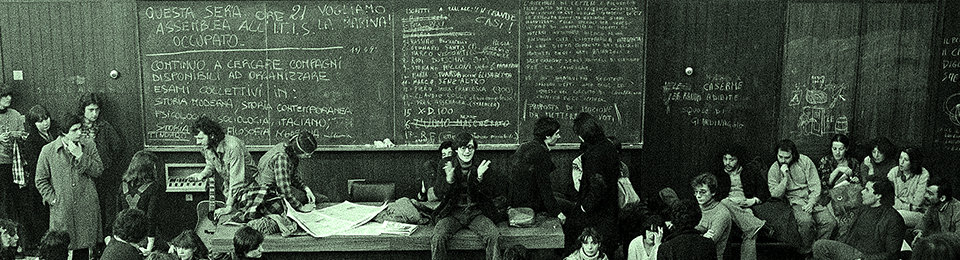
6. The method that the workers used to advance on these levels was that of collective confrontation and of making decisions in assemblies. The assembly of workers in the Policlinico were never moments of ‘irrationality of the masses’ (the most basic level of consciousness), but rather a crucial moment in which the particular synthesises itself within the general: when everyone confronts themselves with everyone the truth about the social relations emerges and it becomes a strength in the moments when the worker faces the doctor or the head nurse alone to oppose their demand for complicity. In the daily assemblies that were organised during the course of struggle, starting from the knowledge about the most basic facts, a collective vision and a political will emerged that took into account the contributions of all workers and at the same time raised the level of political consciousness. [13]
In this way, given the nature of the process that we were analysing, it seemed necessary to use these moments of collective elaboration as the main sources of our inquiry.
As the reader will immediately notice, we used primarily the leaflets, because these reflect the tendency of creating a collective knowledge [tendenza conoscitiva) that we just mentioned. These leaflets were circulated frequently, initially every week and later on, from November 1973, they were produced daily. In this way the leaflets of the ‘Collective of workers’ are a true newspaper, with a capillary distribution in all departments of the hospital, a running commentary on the daily events that, at any occasion, put the workers’ reasoning in front of everyone who believed the in appearances rather than in seeking to analyse reality. They were not an agitatorial instrument of the ‘leading comrades’: their efficiency depended also on the way that they were produced, at the end of an assembly or a meeting, by various comrades who took turns, in a simple and comprehensible language (of the masses and by the masses).
Apart from studying the leaflets, documents and discussion papers we also gathered much material by going to inquiry meetings with the workers and the patients in the hospital and its departments. These were meetings shaped by the necessity to clarify in detail what the changes were that the struggle produced, be it in the balance of power, the balance of power between workers and barons or in the relation between workers and patients. We spoke to workers who were involved in the struggle, but also to those who opposed it; we spoke with patients who understood the need for change, but also to those who “here everyone is a good person, one can see that the professor and consultant are like they ought to be”; with doctors who wanted to “to find a way to do something together with the workers”, but also with other medical professionals who thought that the workers were crazy.
The structure of the book follows both a chronological and argumentative order: at the moment when a struggle broke out, we concentrated on the specific argument or issue of the struggle. At the same time the order of the arguments or issues is not incidental or arbitrary, but is determined by the process of the formation of workers’ consciousness and the way in which they have grasped the functioning of the hospital and the system of power that dominates them. This is a process that is still open and that requires further insights.
The first three chapters describe how the political force of the workers developed around the struggle against the barons and the university hospital, for the unity and equality between workers and the transfer of the management from university to the regional health administration.
The fourth chapter retraces the “five months of exemplary struggle” during which the masses emerged as protagonists of the “proletarian management of the hospital”, resulting in the conquest of the ‘regionalisation’.
The fifth chapter focuses on the new contradictions which appeared between workers and revisionists and the different way in which power relations are being established in the hospital after the regionalisation.
7. There is a final thing to say about our relationship with the workers of the Policlinico. With the work we were doing we did not aim to provide ‘an external service’ for the good comrades who were involved in the struggle, neither did we get involved in it ‘because it was a thing of our group or our party’. [14] We were facing a concrete reality which had the merit to bring to the surface those issues that we have just mentioned: issues that reflect the contradictions that are experienced by workers, all precisely analysed by the workers themselves, many of them confronted, even if they were not all resolved or not always resolved ‘in the best way possible’. We have tried to be part of the internal logic of the popular masses’ movement in order to show, also beyond the horizon of the hospital that this struggle refers to, which difficulties and which challenges they were facing once they decided to advance on the path of their own autonomy and not to entrust their own destiny neither to that part of the big monopolistic bourgeoisie and state that are in power today, nor to the other part that tries to grab power with the help of the popular masses and the wave of their struggle.
For us this work serves to understand how the politics of our movement develops in reality, how it overcomes many obstacles in its way and which are its strong and weak points. It is for all comrades who feel part of this movement, independently from the organisations that they find themselves attached to at this moment, that we want to offer this contribution for reflection.
Footnotes
[1] Marx: Introduction to the Critique of Hegel’s Philosophy of Right (1843) – Furthermore Marx says that the working class is “a class with radical chains” which “has a universal character by its universal suffering and claims no particular right because no particular wrong, but wrong generally, is perpetuated against it”. From here we can draw the necessary conclusion that the working class cannot liberate itself without liberating the entire humanity.
[2] Footnote by translator: In terms of understanding, the comrades use the word ‘barons’ to describe the very elitist, if not semi-feudal character of the medical and university hierarchy at the time. Many of the bosses of the university clinics were embroiled in corruption and had close links with conservative, religious and sometimes fascist circles.
[3] Another preconceived position, which is equally to be combatted even if it is actually less widely spread than the ones that we have mentioned above, is the position of very ‘streetwise’ comrades, who also oppose revisionism and who think that their group or party has the correct line already pocketed – and who participate in the struggle only in order to verify points of convergence and divergence with their line. They don’t bother to subject the experience of struggle to an analysis which would allow them to come to correct political conclusions, which might force them to change their own ideas eventually.
[4] It seems though that this is the way in which Maoist teachings are received within our movement (even though they are then not applied). ‘To engage in inquiry’ has become synonymous with ‘not taking decision-making lightly, weighing up the various aspects of a question’ – a very sacrosanct position which gradually transformed itself into ‘being serious, reasonable, fighting movementism and spontaneity’, thereby forgetting that Mao said: “A Communist Party’s correct and unswerving tactics of struggle can in no circumstance be created by a few people sitting in an office; they emerge in the course of mass struggle, that is, through actual experience.” (Mao Tse-Tung, ‘Oppose Book Worship’
OPPOSE BOOK WORSHIP (marxists.org)
[5] In the presentation ‘Inquiry in the Xing’guo district’, Mao always invoked the necessity to carry out inquiry in the moment of struggle, against the particular deviations of both the right-wing and the ‘left-wing’ of the Communist Party of China.
[6] If we are not taking into account the ‘conditioning’ and its transformations, we will end up endorsing revisionist politics, which only considers the existing conditions in order to maintain them, like a ‘more realistic’ form of politics than ours. This, though, is not more ‘realistic’, but conservative, in the sense that this type of politics tries to adapt itself, whereas only that practice is revolutionary which, starting from the given conditions, tries to overthrow them. (E. Masi, ‘Panzieri e il movimento revoluzionario’, in ‘Aut-aut’ no. 149-50, p.161)
[7] In an article in ‘Rivolta di classe’ from October 1974, which describes the relations between workers and revisionists after the victory that had been obtained with the ‘regionalisation’ of the hospital service, it says: “The true response to these provocations [the spreading of lies and slander by the ‘workers’ party’] is the consciousness and autonomous organisation that workers have been strengthening, and the only relation that they by now have with the trade unions is the constant demonstration of their own power”. This assessment, which is rather triumphalistic, does not take due account of the fact that in this phase the trade union, after having lost a battle, reorganises itself in a different way in order to reconquer its power, precisely by basing its initiative on certain workers, those who are more privileged and less conscious, who constitute the social base of the union.
[8] Most of the anti-institutional literature deals with the contradiction between the power of the institutions and the patients – and this is their merit – while, by doing so, it takes the “complicity” of the workers in the “consensus making” process of the institutions as a given. The same ‘class analysis of the hospital’, which this literature often refers to, tends to become a definition of the class origin of its subjects (doctors = middle to upper bourgeoisie / patients = proletarians etc.) without looking at the conditions from which ‘class struggle in the hospital’ develops. In this way, a book like ‘I diritti del malato’ (The rights of the sick), by G.Bert and others (Feltrinelli, 1975), while providing an extremely clear examination of the class nature of the experience of a patient in a public hospital, it never addresses the proletarian patient as someone who has behind them the power of a class and who can count on the alliance with hospital workers. Therefore, when it comes to the nurses, the book emphasises primarily the tendency of nurses making use of patients’ complaints in their “(ever present) internal rivalries”. In this way the struggle of the patients loses its precise class connotation and ends up locating itself on a purely legalistic plane of a “charter for patient rights” which the institutions are supposed to approve.
[9] Amongst the many things that could be read in recent publications of democratic medicine, it seems that only Jervis provides a coherent analysis of the crucial significance of this factor, without which even the most innovative intervention risks ending up arming revisionism and the monopolistic sector of capital which it sustains. In the introduction of his ‘Manuale critico di psichiatria’ (‘Critical manual of psychiatry’) (Feltrinelli, 1975) Jervis states that in the struggle for health “the role of the working class, be it inside or outside of the factories, is the role of leadership: both because of their own living and health conditions and their organised force and political preparedness”. (p.39) But between words and deeds… we think that only if statements like this find actual application in the struggle of democratic medicine (with the consequence of deepening the struggle also against the trade union leadership of the medical professions) would it be possible to talk about a true alliance between proletariat and democratic medical professionals. Without workers’ leadership – on the contrary – the masses remain the base of yea-sayers [base di consenso] for a sector of progressive intellectuals.
[10] T.W. Adorno, Scritti Sociologici, Torino, Einaudi, 1976, p.346
[11] In this sense there never exists a particular situation in which the general model would not be retraceable. It is only the particular conditions, together with the dialectical capacity of the masses to impact upon them, which allow us to verify an interpretative model. The Policlinico is not a ‘backward’, ‘distorted’ or ‘abnormal’ hospital, nor is the economic development in Italy compared to other capitalist countries.
[12] G.Berlinguer and S.Scarpa (in ‘La riforma sanitaria’, Editori riuniti, 1974) provide the following figures: in Lazio, 32.91% of all hospital beds are in private hospitals, while, in order to make significant examples, in Lombardia the figure is 15.96%, in Emilia 14.64%, in Basilicata
42.10%. The national average is 17.22%, the average in the central north is 15.13%, in the south and Isole it’s 23.20%. Rome, therefore, which largely informs the figures for Lazio, has a high percentage of private hospitals, but it shares this condition with most cities in the south, while the phenomena isn’t absent also in the big cities in the north.
[13] It is political practice, by increasing the level of consciousness of the workers, that also expands their capacity for inquiry. It is not the inquiry itself which raises their consciousness. The assumption by Panzieri that “the method of inquiry has to secure a scientific observation of the ‘level of consciousness’ that the working class has obtained and has therefore also to be the way to ‘lift this consciousness to a higher level’”, seems to require an evaluation from two separate visual angles. It is true, on one hand, that it contains an anti-dogmatic element, which Masi interprets in this way: “The working class are the workers, the new protagonists of history. But only to the degree to which they are aware of it and know how to do it”. But, on the other hand, it also seems to overestimate the political impact that inquiry, organised by groups of comrades, can actually have on the objective conditions of inquiry. But let’s remember that these notes were written in 1964, a bad year for proletarian autonomy, in which vanguard groups like ‘Quaderni Rossi’ were inclined to operate on levels that went beyond what was actually possible.
[14] The main militants of the ‘Collective of workers at the Policlinico’ have always been from the workers’ autonomy in Rome, while those who write this text work within the Centro Stampa Comunista di Roma.